Today during my TR shift, CY asked me for demonstration of how to connect suction canisters in series for large volume paracentesis.
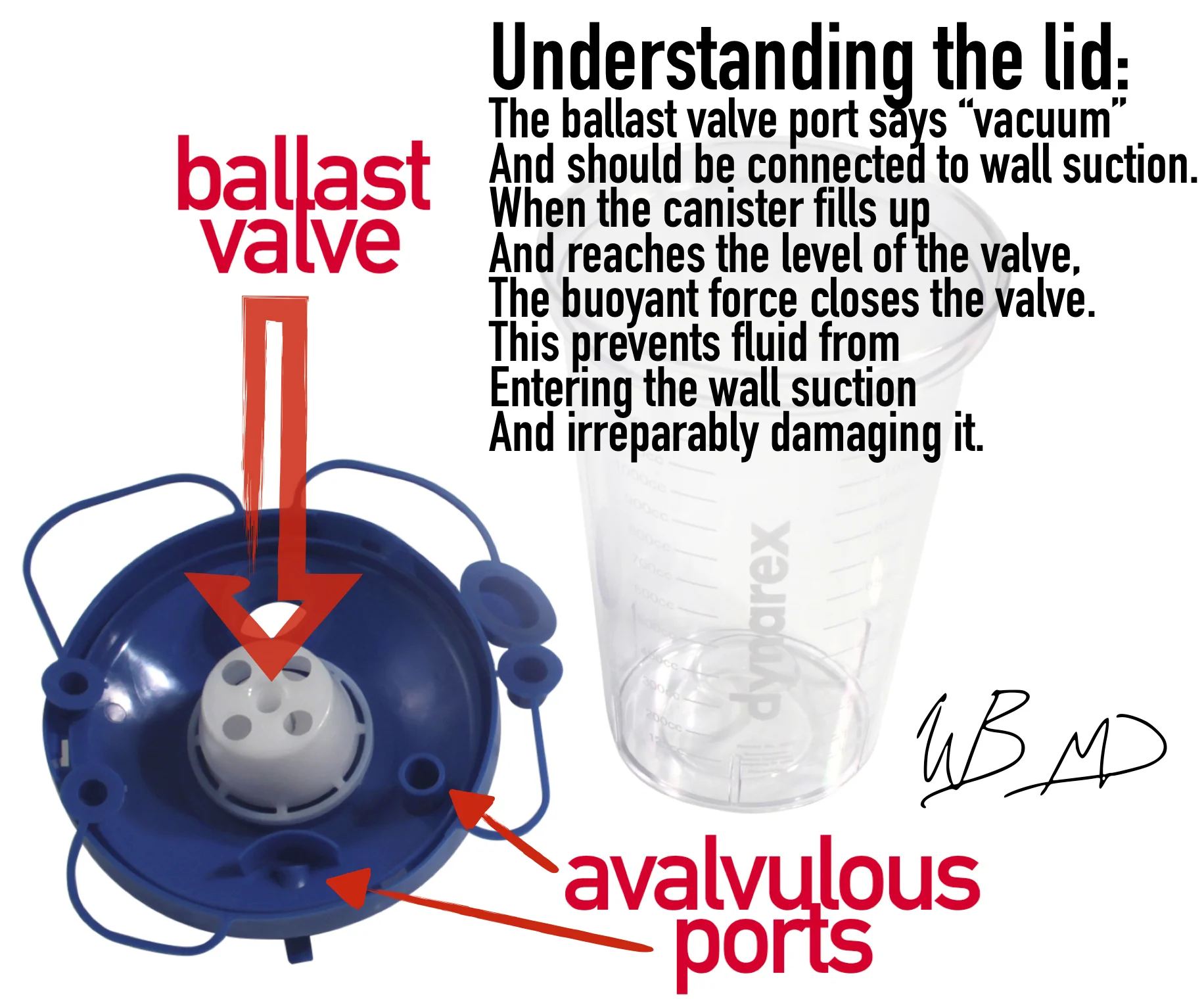
Before we go into the actual technique, lets take a second to understand how the suction canister functions. This is not our exact model of suction canister lid, but is functionally the same. See my infographic below:
The goal: to connect 3 of the vacuum canisters together so that when one fills, the fluid then starts draining into the next. Once the second fills it will drain into third and automatically stop.
With this technique you can perform your paracentesis, start drainage, and then safely walk away. Please instruct your patient not to move whilst drainage is in action.
So connect one suction canister with vacuum tubes as you normally would: vacuum to wall suction; the next vacuum tube should go from either of the avalvulous ports to the next avalvulous port. Critical point: the only port that needs to be connected to the ballast valve port is the port that plugs into wall suction. All subsequent ports should be connected in series with the avalvulous ports.
The final attachment is the avalvulous port to christmas tree adapter, which is included in our thora/paracentesis kit.
During what I believe was my intern year, I had shown Strayer this technique, and much to my chagrin, he tweeted out a post about it. See below:

The benefits of utilizing this technique for large volume paracentesis are twofold: (1) increased safety and (2) utilization of resources (in this case physician time). Safety is increased because this method does not utilize sharp needles to transfer fluid to a vacuum flask; thereby, it reduces the risk of needle stick injury (especially important for the population of patients that need ED paracenteses). Utilization of resources is improved because a physician does not need to remain at bedside or repeatedly check the progress of evacuation, assessing for need to switch to the next vacuum flask.
For large volume paracentesis, I recommend only connecting a max of 4 of our suction canisters in series. I typically do 3, but 4 approaches that max of 5L that current thought suggests may cause hemodynamically significant fluid shifts.