At the request of some of the residents and in light of the case this morning, here’s a review on the Blakemore device for massive variceal bleeding. It can also be used for gastric lavage of acute toxic ingestions for which there is no antidote.
Procedure:
This very well done video on EM:RAP probably describes the procedure better than text:
https://www.youtube.com/watch?v=NHelCd5Jtp4
-Almost all patients will require endotracheal intubation to avoid aspiration.
-All patients require appropriate sedation as you’re passing a giant tube and keeping it there.
-Place in left lateral decubitus if possible to decrease gastric emptying/regurgitation.
-Check the balloons for leaks before starting
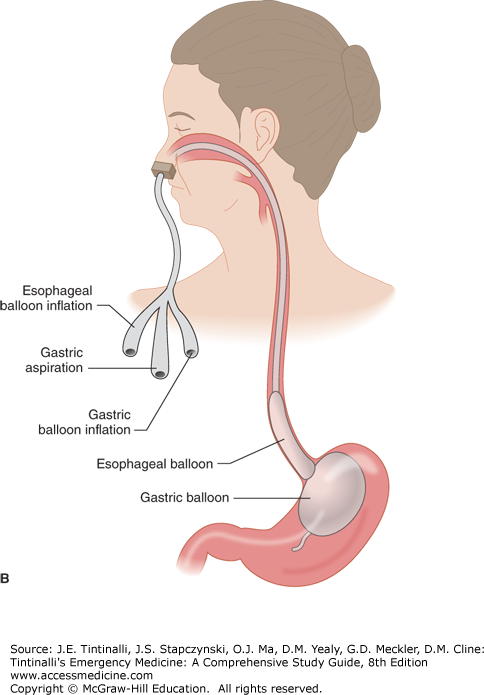
-Pass tube and inflate gastric balloon, it can hold 250 cc’s of air! Get an x-ray to confirm it is in the right place.
-For variceal bleeds, the esophageal balloon should be inflated to about 30mm of mercury pressure. The purpose of the additional OG tube/salem sump in the video is to check for continued bleeding. If there is continued bleeding, the esophageal ballon can be inflated up to 45mm of pressure.
-Through the stomach tube, aspirate all air, water, and blood as subsequent sampling will be an index of the effectiveness of hemorrhage control
-Finally, secure the Blakemore using the method described in the video with kerlex and an IV pole. In our cabinet, we also have a football helmet, see attached image. The concept is the same, to provide enough tension so the Blakemore stays in place.
-Irrigate and aspirate the tube every 30 minutes with 50cc’s of warm water to monitor for worsening bleeding.