POTD: Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy (ARVC)
Case: 22M presents unconscious in VTach. The patient was exercising and suddenly passed out. ACLS performed and after defibrillation, ROSC was achieved. Epsilon wave was seen on EKG, pt was admitted to MICU, which did MRI showing arrhythmogenic RV dysplasia.
Arrhythmogenic Right Ventricular dysplasia:
Inherited myocardial disease where R ventricular myocardium is replaced by fibro-fatty tissue
Typically autosomal dominant but there is recessive form caused Naxos Disease with wooly hair and skin changes
3:1 men to women, more in Italian or Greek descent, 1:5000 people overall
Second most common cause of sudden cardiac death to HOCM (causes 20% of sudden cardiac death in pt < 35yo)
Presentation: 30-50s with syncope or dysrhythmias including PVCs, VT, VF, CHF, or sudden cardiac death
EKG:
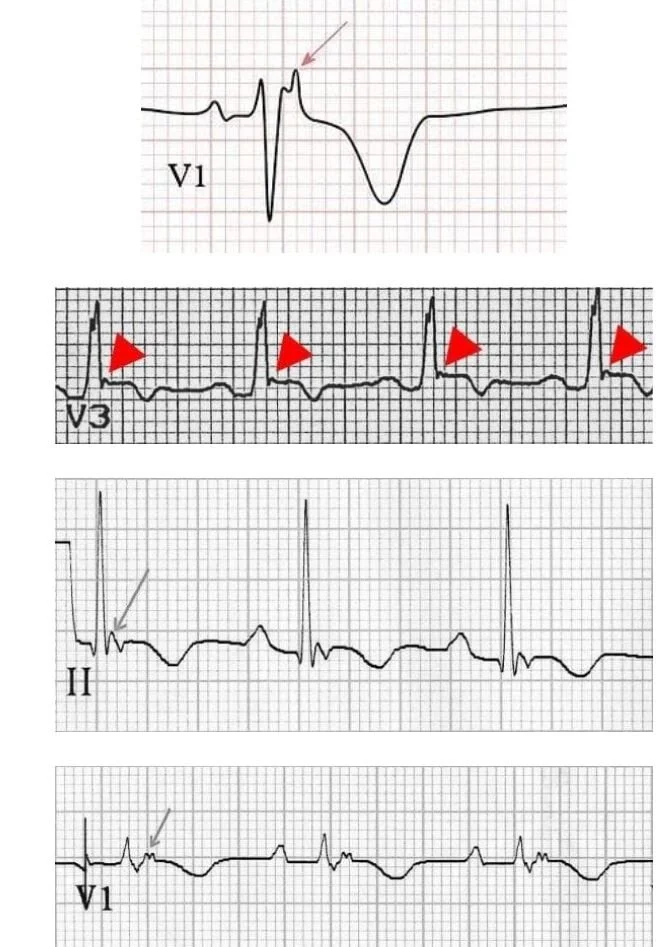
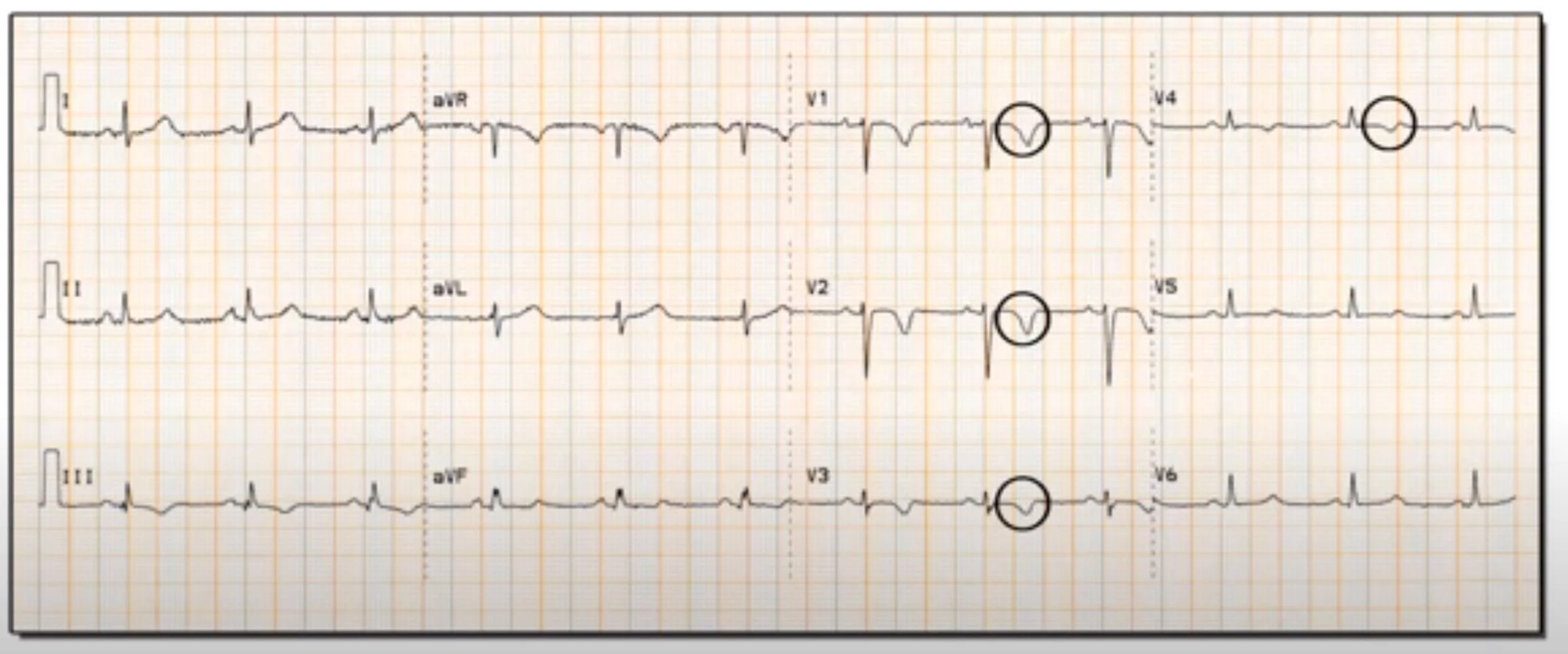
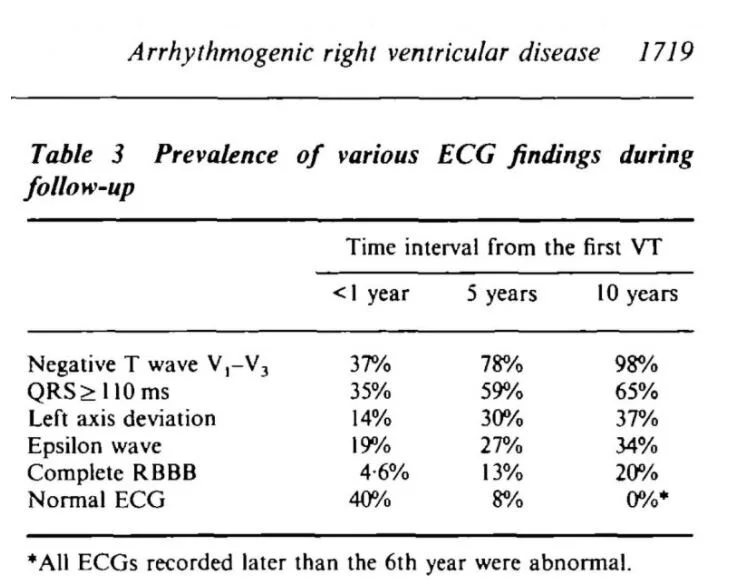
Epsilon waves are the most specific finding on EKG (30-50% spec) but there are other findings as well, the most common being TWI in V1-V3. The epsilon wave occurs because conduction is slower through fattier tissue, and there is a post-excitation wave.
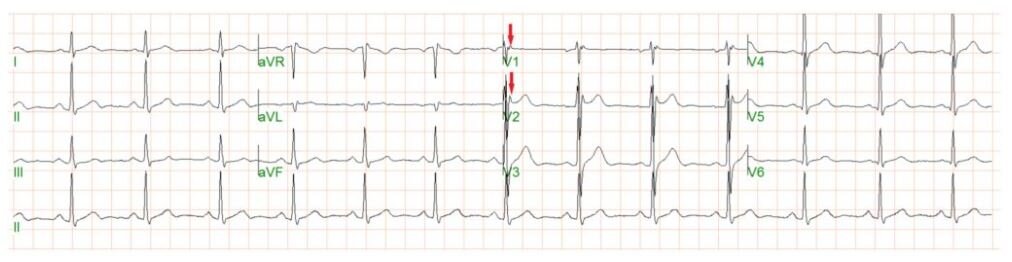
It can be difficult to pick up epsilon waves, a different set of lead placement can be used
RA over manubrium, LA over xiphoid, LL in V4 position, I/II/III will be denoted as FI/II/III in the image

Imaging:
Echo – dilated hypokinetic RV with prominent apical trabeculae and dilated RV outflow tract
MRI – will see fibrofatty infiltration, RV dilation, wall motion abnormalities
Treatment:
Betablockers preferably Sotalol or amiodarone
ICD placement if patient has sypmtoms, some pathways can be ablated
Some patients will develop heart failure and will require standard CHF treatment, other might need heart transplant
Disposition:
If patient is asymptomatic and abnormal EKG is found incidentally, the patient can be discharged with cardiology f/u
The patient should be admitted if concerning symptoms likely syncope, chest pain, arrhythmias or has a family history of sudden death/cardiac arrest