Ankle fractures:
Start with good H&P:
History:
Mechanism, height of the fall, direction of the foot inversion
Consider age, steroid use, hx of neoplasm, prior surgeries, hardware
Physical:
Start from the knee down, neurovascular intact, ROM, strength, severe tenderness, instability, rash/ulcers
Classification of the injury: stable/unstable?
Many classifications are available but for ED we can use Closed Ring System:

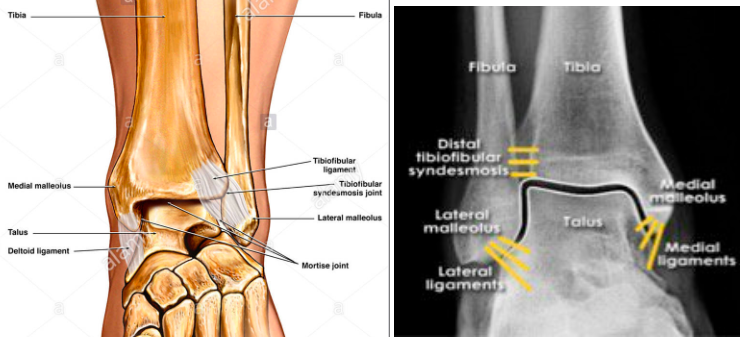
Think of an ankle as a ring of bone and ligaments surrounding the talus consisting of the tibia, the medial malleolus and medial deltoid ligaments, the fibula and lateral ligaments and calcaneus.
A single disruption in the ring - stability most likely preserved
Two disruptions - think instability and will likely cause the joint to shift.
Exceptions: Lateral malleolus fracture even with no medial injury may become unstable.
Isolated syndesmosis injury
Approach to ankle injuries x-ray interpretation
Here is an EM focused summary
Look at the cortical disruption of each bone
Look at the soft tissue swelling
Look at the spaces between the bones
Look within the bones
Ask for a mortise view (no, it’s not a GOT character) in addition to the standard AP and lateral views
Look at the tib/fib, knee and base of the 5th metatarsal
Key areas:
Talar shift: look to make sure there is congruence between the clear space on either side of the talus; go further - measure the medial clear space and the lateral clear space. If they are incongruent or the medial clear space is >4mm the ankle is likely unstable.
Talar tilt: The lines in red below should be parallel. Talar tilt indicates an unstable ankle

Just a few commonly missed fractures at the ED:
High ankle sprain: The isolated syndesmosis injury - isolated distal tibiofibular syndesmosis injury, with ligamentous disruption can result in unstable ankle injury.
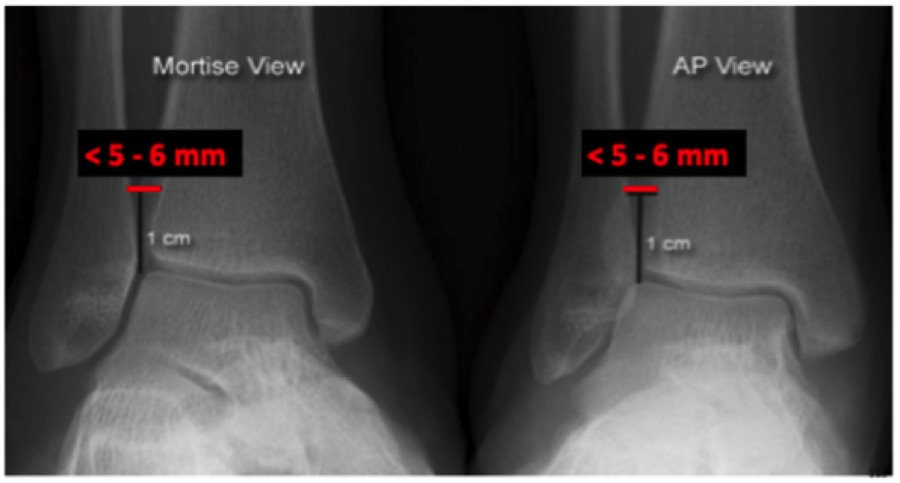
Look at the tibio-fibular clear-space: Measure the gap between the tibia and fibula 1cm proximal to the tibial plafond on both the AP view and mortise view. They should be <6mm. If >6mm, suspect a syndesmosis injury.
Tillaux fracture - fracture is an intra-articular Salter-Harris class III fracture of the distal tibia with avulsion of the anterolateral tibial epiphysis.
Remember that in children, the ligaments tend to be stronger than the growth plate. Tillaux fractures can be considered “the syndesmosis injury of children”

Snowboarder’s fracture - A snowboarder’s fracture is a lateral process of the talus fracture that is commonly misdiagnosed as a simple ankle sprain.

Lateral process of the talus fracture also known as a snowboarder’s fracture
Bottom line:
Reassess including the if the pt is still neurovascular intact
If pt can’t ambulate get further workup
If in doubt call radiology
Persistent pain but pt wants to go hoe, splint with ortho follow up
References: CoreEM, EMDoc, Uptodate, Radiopedia