When to perform it?
· To release orbital compression syndrome, most commonly due to retrobulbar hematoma.
· IOP > 40, the pressure that indicated that you need to cut and release the compartment syndrome.
· Without decompression, irreversible vision loss due to increasing orbital pressure may occur in as little as 90-120 minutes.
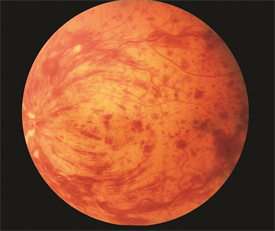
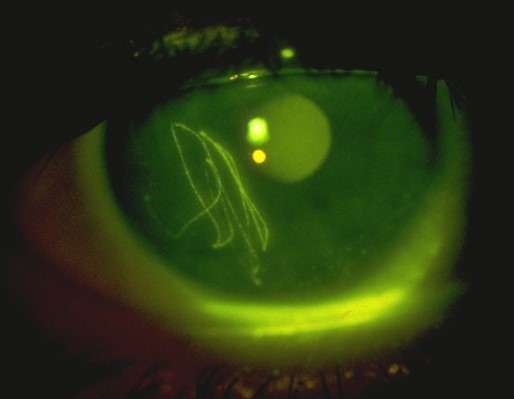
Clinical situation: trauma to the head/face.
Physical exam:

https://www.emra.org/emresident/article/emergency-department-evaluation-of-blunt-orbital-trauma/
CT head and face

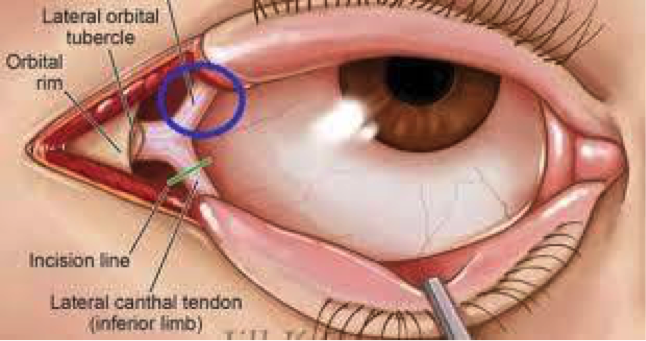
familiarize yourself with the anatomy
Before starting, highly consider sedation.
Steps:
1) Generously inject 1% Lidocaine with epi to numb that lateral canthus to the orbital rim.
Do this by directing the needle away from the globe itself
Helps with bleeding and with pain.
2) Using the needle driver as your hemostat, advance from the lateral canthus to outer orbit rim. Clamp down and hold for 1- 2 minutes.
3) Using your small scissors, cut the lateral canthus to the orbital rim.
4) Then cut inferiorly to cut the inferior crus of the lateral canthus (you may need to probe around to feel the structures)
5) Repeat IOP. If the IOP is not immediately lower, then cut the superior crus of the lateral canthus and recheck pressure.
Pearls:
· There is a lot of swelling. It can be hard to fit your hemostat in place and to feel your landmarks. Use you instruments to feel/probe around.
· Also, do not worry about cutting too much. You are doing this to save this patient’s vision. After discussing this with optho, these are repaired quite easily days/weeks later. For example, Dr. Tome Levy performed this once on a patient that I later followed up with in split flow about 2 weeks later. There was no physical evidence on physical exam that this had ever happened. At first I thought I had the wrong patient in front of me… but the patient confirmed that a week and half ago he had in fact had the optho plastic surgery to repair it.
Sources:
https://emedicine.medscape.com/article/82812-overview
http://www.tamingthesru.com/blog/annals-of-b-pod/ocular-emergency
This is an excellent emrap video that reviews the procedure: https://www.youtube.com/watch?v=tgQaKVGynFA