Diagnosis:
new-onset tonic-clonic, focal, or multifocal seizures in the absence of other causative conditions (eg, epilepsy, cerebral arterial ischemia and infarction, intracranial hemorrhage, drug use),
typically but does not have to be present in the presence of preexisting hypertensive disorder of pregnancy (preeclampsia, gestational hypertension, HELLP syndrome)
Presentation:
Hypertension
Headache (persistent frontal or occipital headaches or thunderclap headaches)
Visual disturbances (scotomata, loss of vision [cortical blindness], blurred vision, diplopia, visual field defects [eg, homonymous hemianopsia], photophobia)
Right upper quadrant or epigastric pain
Asymptomatic
Management:
Start with ABCs
Consider alternative causes of seizures based on additional information other than eclampsia: hyponatremia, ICH, hypoglycemia, etc.
Usually eclamptic seizures subside on its own
If pt is seizing => administer Mg Loading dose 4-6 g IV over 15 to 20 minutes. An alternative dose/route is magnesium sulfate 5 g intramuscularly into each buttock for a total of 10 g
Followed by Maintenance dose – magnesium sulfate 2 g/hour as a continuous IV infusion to women with good renal function.
If pt is in status => in cases refractory to magnesium sulfate (patient is still seizing at 20 minutes after the bolus or more than two recurrences), administer sodium amobarbital (250 mg IV over three minutes), thiopental, or phenytoin (1250 mg IV at a rate of 50 mg/minute). In this case pt will need to be intubated.
If need to consider intubation:
Medications:
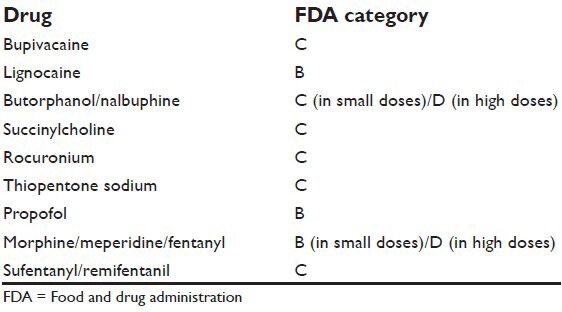
Induction - consider propofol (category B)
You want to avoid: Etomidate - lowers seizure threshold and Ketamine - worsens HTN
Paralytics - rocuronium or succinylcholine, yet both of the medications are category C so use minimal dose to reach the desired effect, avoid additional doses
Next consider hypertensive control if BP diastolic pressures greater than 105 to 110 mmHg or systolic blood pressures ≥160 mmHg:
Labetalol - 20 mg IV gradually over 2 minutes.
Hydralazine - 5 mg IV gradually over 1 to 2 minutes.
Nifedipine immediate release - 10 mg orally.
Nicardipine (parenteral) - The initial dose is 5 mg/hour intravenously by infusion pump and can be increased to a maximum of 15 mg/hour.
Proceed with labs, consider HELLP syndrome labs, type and screen, fluids.
Call OB/GYN early
The definitive treatment for eclampsia is prompt delivery.

